



The Power of Distraction

We often think of distractions as negative. We may get distracted by all the to-dos on our list, and it’s hard to stay focused on work or give our full attention to someone. Our kids may get distracted while getting dressed, or for older kids maybe it’s while doing homework. But let’s reframe distractions. They […]
Acupuncture for Anxiety: Podcast Episode #105
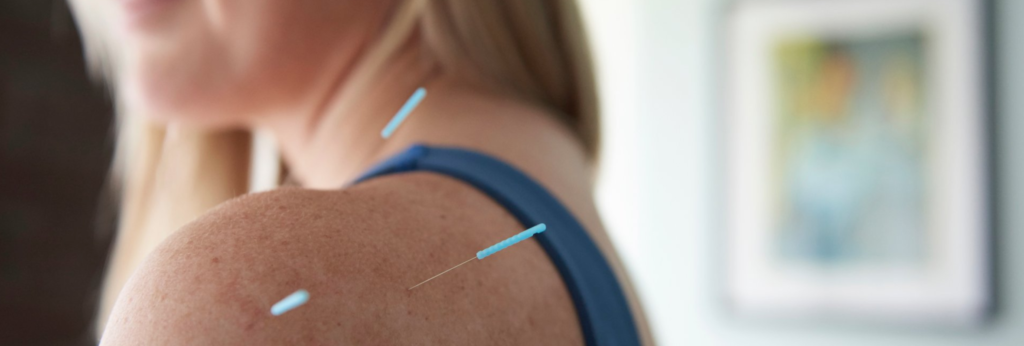
Kristin Revere, Co-Owner of Gold Coast Doulas talks with Vikki Nestico of Grand Wellness about acupuncture to help relieve stress, tension, and anxiety. You can listen to this complete podcast episode on iTunes or SoundCloud. Kristin: Welcome to Ask the Doulas with Gold Coast Doulas. I’m Kristin, and I’m here today with Vikki from […]
Hyperemesis Gravidarum

This post was written by Lauren Utter, a ProDoula trained Birth and Postpartum Doula with Gold Coast Doulas. Finding out you are pregnant can bring an array of emotions – planned pregnancy or not. Maybe you’re excited because you have been waiting for this day. Maybe you are surprised because a baby wasn’t on your […]
Adult Separation Anxiety: Podcast Episode #99

On this episode, Alyssa and Laine begin by talking about parenting anxiety and the distance that parents can sometimes feel as their babies and children grow and seem to need them less. The conversation takes some interesting turns to talk about having clear boundaries for kids, pivoting our expectations of children as they grow, and […]
Parenting and Sleep: Podcast Episode #98

Laine Lipsky, Parenting Coach, talks with Alyssa today about the negative effects of sleep deprivation on children and parents. You can listen to this complete podcast episode on iTunes or SoundCloud. Alyssa: Hello and welcome to the Ask the Doulas Podcast. I am Alyssa Veneklase. I’m excited to be back with Laine Lipsky, parenting coach. […]
Mental Health Awareness Month: Podcast Episode #97

Dr. Nave now works with queens through her virtual practice Hormonal Balance. Today she talks to us about hormones and how they affect our mental health, including the baby blues and postpartum depression. You can listen to this complete podcast episode on iTunes or SoundCloud. Alyssa: Hi. Welcome to Ask the Doulas Podcast. I am […]
Perinatal Mood Disorders: Podcast Episode #91

Today we talk with Elsa, a therapist at Mindful Counseling in Grand Rapids, Michigan who specializes in perinatal mood disorders. Learn what postpartum anxiety and depression look like, how they are different, and signs to look out for. You can listen to this complete podcast episode on iTunes or SoundCloud. Kristin: Welcome to Ask the […]
Stress Mastery: Podcast Episode #85

Deb Timmerman, RN, DAIS, CSME speaks with us today about her new certification in Stress Mastery. What does that mean, you ask? It’s all about learning positive ways to handle stress and actually master it, instead of letting stress take over. Listen to see how this can help parents throughout pregnancy and postpartum. You can […]
How Sleep Deprivation Impacts New Parents

Becoming a parent is one of the most exciting and scary milestones of a person’s life. It’s likely your emotions will run the gamut from excited anticipation and joy, to fear of the unknown and uncertainty about what’s ahead and how you’re coping with parenthood. Managing night time feeds, tending to your baby throughout the […]
Supporting a Postpartum Mother: Podcast Episode #79

Elsa Lockman, LMSW of Mindful Counseling talks to us today about how partners, family members, and other caregivers can support a mother during those critical postpartum weeks to ensure she seeks help if needed. How do you approach a new mother and what are her best options for care? You can listen to this complete […]
Benefits of A Postpartum Doula and Why Should You Hire One?

Author Bio: Roselin Raj is a journalist and a writer. She has been writing extensively on health and wellness related topics for over a decade. Besides her professional interests, she loves a game of basketball or a good hike in her free time to fuel her spirits. “Health is wealth” is one motto of life […]
EMDR Therapy: An Overview

We are so excited to share this guest blog by Joshua Nave LLMSW and Paul Krauss MA LPC of Health for Life GR. We get asked frequently about EMDR Therapy, so read below to find out what it is and how it works! This blog is a discussion of the basics of what Eye Movement […]
Podcast Episode #68: Overnight Doula Support
Many of our clients and listeners don’t fully understand what overnight doula support looks like. Kristin and Alyssa, both Certified Postpartum Doulas, discuss the kinds of support their clients look for and how their team of doulas support families in their homes. You can listen to this complete podcast on iTunes or SoundCloud. You can […]
Podcast Episode #62: Newborn Traumas

What is birth trauma and do all babies experience it? How can you remedy it? Dr. Annie and Dr. Rachel of Rise Wellness Chiropractic give us several examples of common birth traumas, what they mean, and how chiropractic care can help. You can listen to this complete podcast episode on iTunes or SoundCloud. Kristin: Welcome […]
Podcast Episode #60: A Naturopath’s Perspective on Pregnancy and Depression

Doctor Janna Hibler, ND talks to Alyssa and Kristin about how a naturopathic doctor treats pregnant and postpartum women, body and mind. You can listen to this complete podcast episode on iTunes and SoundCloud. Alyssa: Hello, welcome to Ask the Doulas podcast. I am Alyssa Veneklase, co-owner of Gold Coast Doulas, and I am here […]
Media – Friend or Foe?

In light of recent events, we have a special guest blog by Lindsey Zaskiewicz, LMSW. Lindsey is a licensed social worker currently employed as a clinician on a mental health and substance abuse crisis line. Prior to this role, she has several years of experience working in maternal-infant mental health, as well as direct practice with […]
Postpartum Depression & Anxiety Resource List

After our recent event at the Wealthy Street Theatre where we screened ‘When the Bough Breaks – A Documentary about Postpartum Depression’ we realized that there are many great resources available to our community, but people may not know how to find them. We at Gold Coast, with the help of Cristina Stauffer, have compiled […]
